Who is this guideline for?
This guideline provides information on female genital mutilation as a tradition and guidelines for practical, preventive work. The guideline is intended for professionals in the healthcare and social welfare sectors, early childhood education and care and education, and other professionals who encounter the phenomenon in their work. The guidelines include recommended measures.
What is female genital mutilation?
Female genital mutilation is a form of violence against women. Female genital mutilation, or female circumcision or cutting, refers to all procedures that involve the partial or total removal of, or injury to, the external female genitalia for non-medical reasons. The abbreviation FGM is also used to refer to "female genital mutilation".
In most cases, female genital mutilation occurs when a girl is between the ages of 0 and 15. The age at which female genital mutilation is performed varies greatly from country to country, region to region, and ethnic group to ethnic group.
The World Health Organization (WHO, 2008) classifies female genital mutilation into four different types:
- Type I: Removal of the visible clitoris and/or the clitoral hood.
- Type II: Removal of the visible clitoris and inner labia. The outer labia may or may not be cut.
- Type III: Cutting of the inner and/or outer labia and joining of the cut labia so that only a small opening remains for the passage of urine and menstrual blood. The visible clitoris may be removed or covered by tissue that narrows and constricts the vaginal opening. This procedure is called infibulation or pharaonic circumcision.
- Type IV: All other harmful procedures to the female genitalia performed for non-medical reasons. These include pricking, piercing, incising, scraping, and burning with a hot iron.
In practice, it can be difficult to distinguish between the types of FGM, as various mixed forms are common.
Female genital mutilation has no health benefits. Instead, it can cause a variety of physical and psychological harm, such as pain, infections, urinary problems, sexual problems, and complications during childbirth. The harm caused depends on factors such as who performs the procedure, how it is performed, the extent of the mutilation, and the conditions under which it is performed.
Immediate health risks
Pain, heavy or prolonged bleeding, which can lead to anaemia, shock, or death; difficulty urinating; urinary tract infections; infections; viral infections (e.g., hepatitis B and C, HIV); damage to other tissues and organs during mutilation, bone fractures and dislocations caused by restraint, psychological problems: fear, stress, nightmares.
Long-term health problems
Pain, especially during menstruation, urination, and intercourse; difficulty urinating; urinary tract infections; urinary incontinence; consequences of scarring: accumulation of menstrual blood in the vagina; cysts and tumours, tissue inelasticity, fistulas (abnormal openings) to the bladder and intestine, challenges with gynaecological examinations, fear of intercourse, pain during intercourse, inability to have intercourse due to sutured genitals, orgasm problems, infertility, psychological problems, post-traumatic stress disorder, nightmares, insomnia, eating disorders, cognitive disorders, low self-esteem, anxiety, depression.
Problems related to childbirth
Difficulties in monitoring labour and foetal well-being, prolonged pushing stage, tears, bleeding, infections, perineal incision (episiotomy), caesarean section, transmission of chronic infections from mother to child (e.g. hepatitis B and C, HIV), psychological problems: fear of childbirth, flashbacks of mutilation, reluctance to give birth again.
There are many reasons behind female genital mutilation:
- Cultural: The tradition is seen as part of identity and community continuity.
- Religious: No religion requires female genital mutilation, but it is practised in various religious communities.
- Moral: FGM is believed to ensure virginity and increase eligibility to marry.
- Purity-related: FGM is believed to be a form of “purification” that protects against disease.
- Aesthetic and sexual: Girls who have undergone FGM are considered beautiful and sexually restrained.
- Economic: A daughter who has undergone FGM can bring a dowry to the family.
- Social: Community pressure and fear of discrimination can force families to continue the tradition.
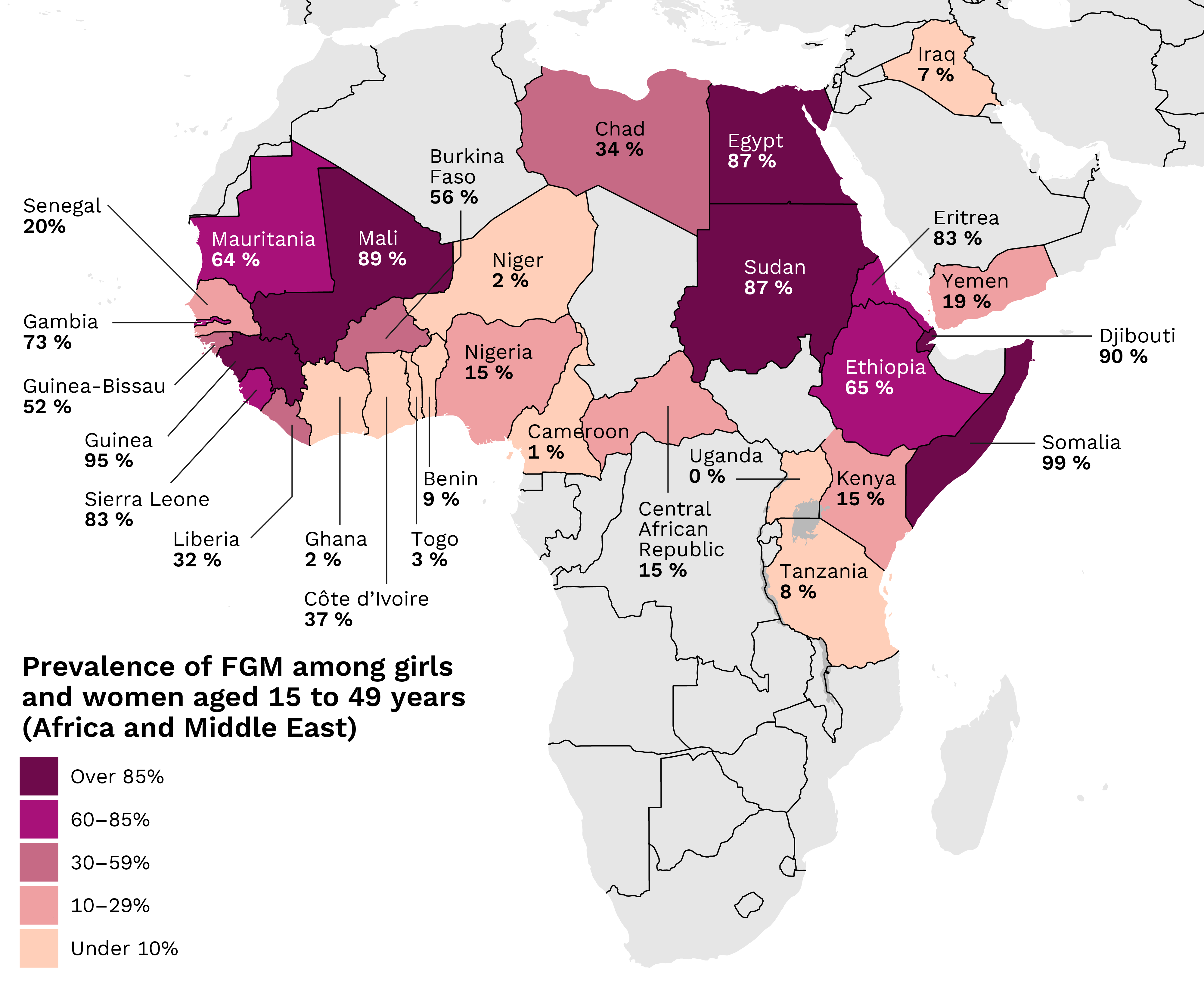
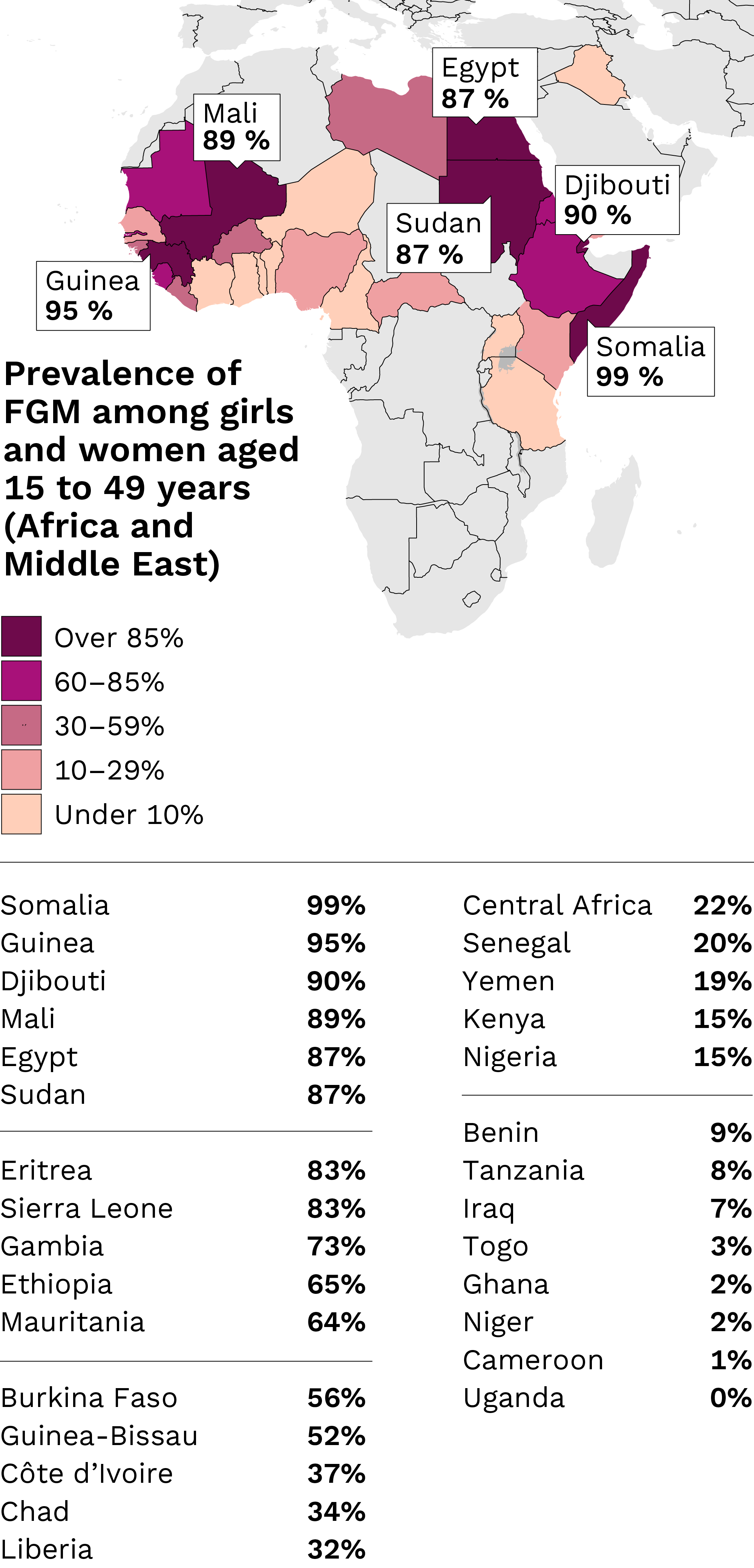
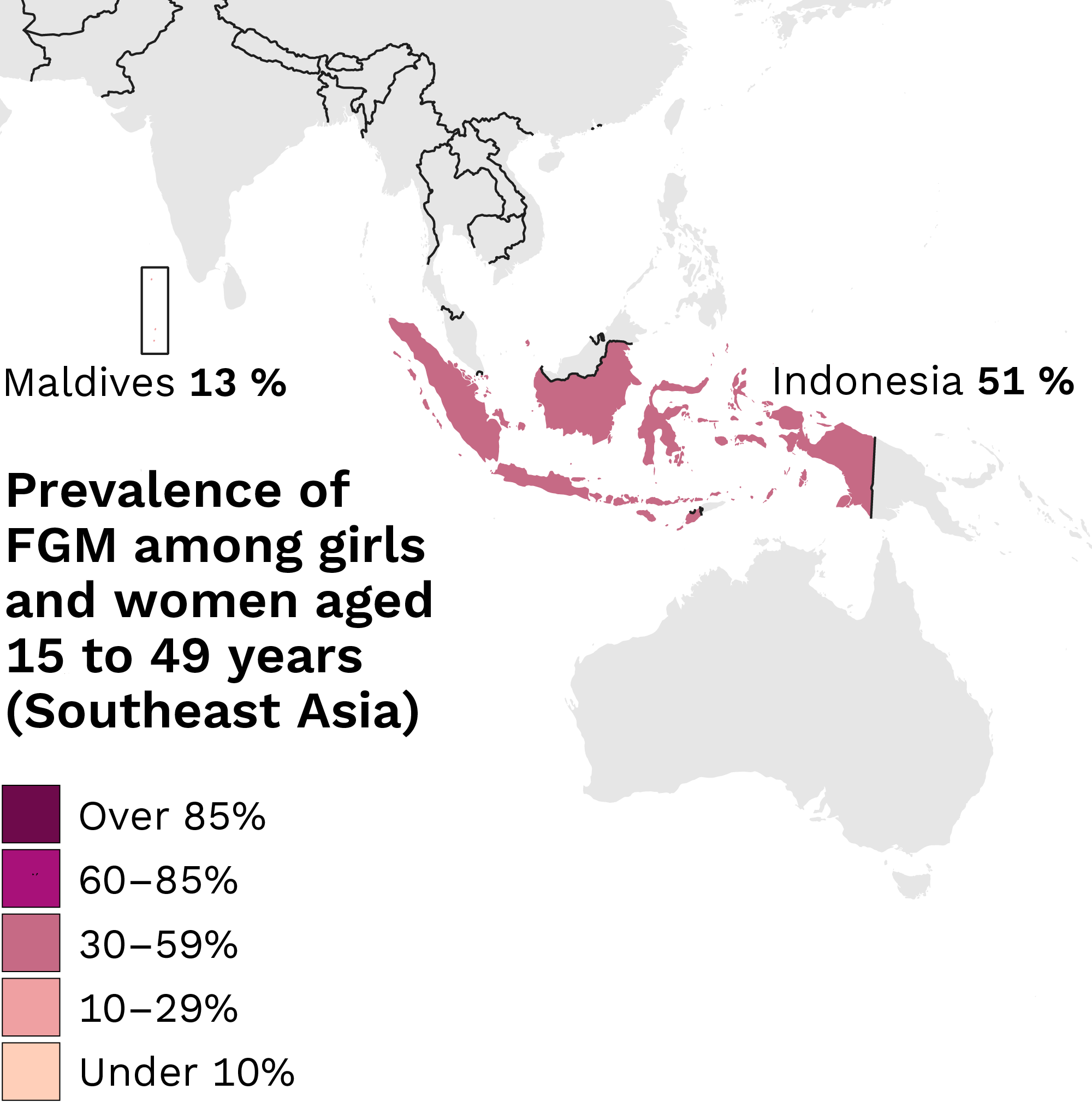
It is estimated that there are currently 230 million girls and women around the world who have undergone female genital mutilation. Every year, approximately four million girls are at risk of being subjected to female genital mutilation. The prevalence of female genital mutilation varies from region to region. Countries with high prevalence rates include Somalia, Guinea, Djibouti, Mali, Egypt and Sudan. FGM is also practised in the Middle East and Asia. The practice is most common in countries where it is considered a cultural tradition.
Prevalence of FGM among girls and women aged 15 to 49 years (Africa and Middle East)
Prevalence of FGM among girls and women aged 15 to 49 years (Southeast Asia)

Source
UNICEF. Female genital mutilation (FGM). Global Databases. 2025.
Related information
Traditions and a harmful practice (Youtube)
FGM is a crime
Female genital mutilation (FGM) violates several international human rights conventions to which Finland is committed. Female genital mutilation and any related preparations are punishable acts under the Criminal Code of Finland:
According to the Criminal Code, FGM can result in a prison sentence of 1–10 years. In addition, preparation of FGM can lead to imprisonment for four months to five years.
(Criminal Code, Chapter 21, Sections 6 b and 6 c)
- Incitement, coercion and assistance, such as sending a child to another country for genital mutilation, are also crimes.
- The statute of limitations for prosecution related to FGM is 20 years. If a minor girl has undergone FGM, the limitation period begins when she turns 18.
- If a Finnish citizen or a person comparable to one, such as a foreign national permanently residing in Finland, commits FGM abroad, the act is punishable even if it is not considered a crime under the laws of that country.
Criminal Code of Finland, Chapter 21: Homicide and bodily injury (in Finnish, Finlex)
The risk of FGM may constitute grounds for international protection, and all asylum seekers must be asked about FGM during their initial health examination.
How to ask about FGM during an initial assessment (in Finnish, Youtube)
Suspected FGM
If you suspect that a girl has undergone FGM while living in Finland or that preparations for FGM are ongoing, report it to the child welfare services and the police
The same guidelines apply to suspected FGM as to reporting any other forms of violence. If you are unsure whether FGM meets the criteria for mandatory reporting in a child’s situation, consult the police, child welfare services or a forensic psychology centre.
In some situations, involving child welfare authorities and the police may create a risk of the family leaving the country before help can be arranged for the child. Therefore, it is important that child welfare services and the police investigate the situation before the guardians are informed that a report has been filed. If necessary, border authorities may prevent the family from leaving the country.
In case of a suspected offence, the police or child welfare services first meet the child and then each guardian separately. Guardians are only met if it is confirmed that the matter may be disclosed to them. Meeting guardians separately makes it more likely for family members to speak more openly about issues they may be hiding from each other. The risk must be assessed for all children in the family.
In unclear situations, it is appropriate to consult child welfare services or the police. For example, when:
- FGM has probably been carried out abroad before the family’s arrival in Finland.
- A girl who has already undergone FGM has a younger sister in the same family.
Notifying female genital mutilation (FGM)
Guidelines on the exchange of information between healthcare and the police (in Finnish, Valto)
Addressing FGM
Female genital mutilation is a sensitive topic that can feel difficult to raise. However, it is important to do so as early as possible. Addressing the issue is the most effective form of preventive work.
It is important to remember that FGM is considered a normal and respected practice in specific cultural contexts. In a new environment, girls and women who have undergone FGM may feel different, which can make them anxious about meeting a professional.
How to raise the topic of FGM?
Bring up FGM, for example, before long holidays when families may travel abroad to their former home countries. Remind the family that relatives and acquaintances may suggest FGM for the girl. If, after a trip, there is suspicion that FGM has been performed, investigate the matter.
When talking with the client, it is best to use the term the client themselves uses, such as “circumcision” or “cutting”.
Make it easier to address the topic by:
- having the issue listed in the client’s pre-information form
- explaining that the next discussion will cover intimate and sensitive matters
- using ready-made phrases for professionals to clarify the issue
- informing the client that the professional is obliged to ask about the matter
- opening the discussion with cultural or family traditions
You can ask the client, for example:
- Which country are you from? Which country is your family originally from?
- Do you know what female genital cutting means?
- According to the map, female genital cutting is common in your country of origin. How is the practice viewed in your family or community?
- Have your mother or your sisters been subject to female genital cutting? What about you?
- How do you intend to act regarding your own daughter?
In preventive work, it is essential to understand the tradition of FGM and its prevention as part of combating violence. As a professional, your task is to raise the topic in a confidential and culturally sensitive way at maternity and child health clinic appointments or in school and student health care, especially when discussing changes related to puberty. Address the issue with children and young people in an age-appropriate manner.
Explain the health risks, offer support, explore parents’ attitudes, inform them that FGM is illegal and, if necessary, file a child welfare notification and a police report. Document all discussions. In unclear situations, consult the authorities and always prioritise the child’s safety.
Early childhood education and care works in cooperation with child health clinics and child welfare services, and managers in early childhood education and care must ensure that staff are also knowledgeable about this topic. Raise the issue with parents, for example, during discussions about the early childhood education and care plan and before longer holidays to countries where FGM is practised. All children have the right to physical integrity and health.
FGM risk assessment form
You can use the FGM risk assessment form in the discussion with the client. The form includes a map of countries where FGM is more prevalent. You can also use supporting questions to make the discussion easier.
The form in different languages:
- FGM risk assessment form (in English)
- FGM risk assessment form (in Finnish)
- FGM risk assessment form (in Swedish)
Materials for addressing FGM and raising the topic
- What does FGM mean and how to support a client who has experienced it (in Finnish, Youtube)
- What does FGM mean and how to support a client who has experienced it (In Kurdish Soran, Youtube)
- How to raise the topic of FGM (in Finnish and in Somali, Youtube)
- Preventing and addressing female genital mutilation in child health clinics (in Finnish, Julkari)
- Preventing female genital mutilation in school and student health care (in Finnish, Julkari)
THL’s role
THL is a national expert in violence prevention. We support wellbeing services counties and professionals in social and health care by providing guidelines, recommendations, tools, and training. We also develop structures for violence prevention and coordinate collaboration in the field.
Contact details

Senior Specialist
tel. +358 29 524 7554
[email protected]
Specialist
[email protected]